Empathy in Action: Enhancing Cancer Care Through the Expertise of Oncology Nurses

Oncology nurses are at the heart of cancer care. They provide more than just medical expertise—they offer empathy, compassion, and support during some of the most challenging moments in a patient’s life. But what does empathy look like in action, and how can oncology nurses channel it for better patient care while protecting their own well-being?
This post explores the role of empathy in cancer care, its impact on nurses and patients, and actionable strategies to transform empathy into meaningful, measurable improvements in care environments.
What Is Empathy in Cancer Care?
Empathy in cancer care goes beyond understanding a patient’s condition. It involves recognizing their emotional, physical, and psychological struggles while providing care that addresses those needs holistically.
For oncology nurses, this means listening attentively to patients, validating their fears and hopes, and translating those insights into compassionate, personalized treatment. Empathy bridges the emotional gap in patient care, transforming clinical relationships into human experiences.

The Dual Impact of Empathy in Oncology Nursing
While empathy is essential, oncology nurses often walk a fine line between caring for others and safeguarding their own well-being. Positive nurse and patient experiences are crucial as they are linked to a range of beneficial outcomes.
The Benefits of Empathy
/ Better Patient Outcomes: Cancer patients often face fear and uncertainty. An empathetic approach helps establish trust and reduces emotional barriers between patients, their families, and caregivers. This trust leads to open communication, creating a collaborative care environment. 1 Empathic care leads to higher patient satisfaction scores, reduced stress levels, and improved adherence to treatment plans. Research shows that empathy in healthcare leads to better treatment adherence and improved patient satisfaction. When patients feel understood, they are more likely to follow care plans and share vital health concerns, leading to better outcomes. 2
/ Positive Feedback Loops: For many cancer patients, the relationship with their oncology nurse becomes a source of comfort and stability. Empathy fosters a deeper connection, turning routine care into a reassuring and supportive experience. Patients who feel valued often express gratitude, boosting job satisfaction and reinforcing the importance of empathic care.
/ Enhanced Team Morale: When nursing teams adopt empathy as a shared value, it fosters a collaborative atmosphere, reducing burnout and improving team dynamics.
/ Stronger financial performance: Workplaces that prioritize empathy foster more positive environments, resulting in higher employee retention, reduced burnout, and fewer cases of illness.
The Challenges of Empathy
/ Nursing Burnout: Constant emotional engagement with patients can lead to caregiver fatigue and burnout. Many patients endure severe pain or recieve palliative care, and over time, the emotional burden on nurses takes a significant toll.
/ Pressure to Balance: Nurses must juggle technical responsibilities with compassionate care, which can feel overwhelming.
A New Perspective on Empathy in Action
Empathy often requires time and focus, both of which are precious commodities in an oncology nurse’s day. Empathy isn’t a one-way street. To provide exceptional care to their patients, oncology staff need the support they rightfully deserve. One innovative way to ensure this is by incorporating CSTDs into their workflow.
What Are CSTDs?
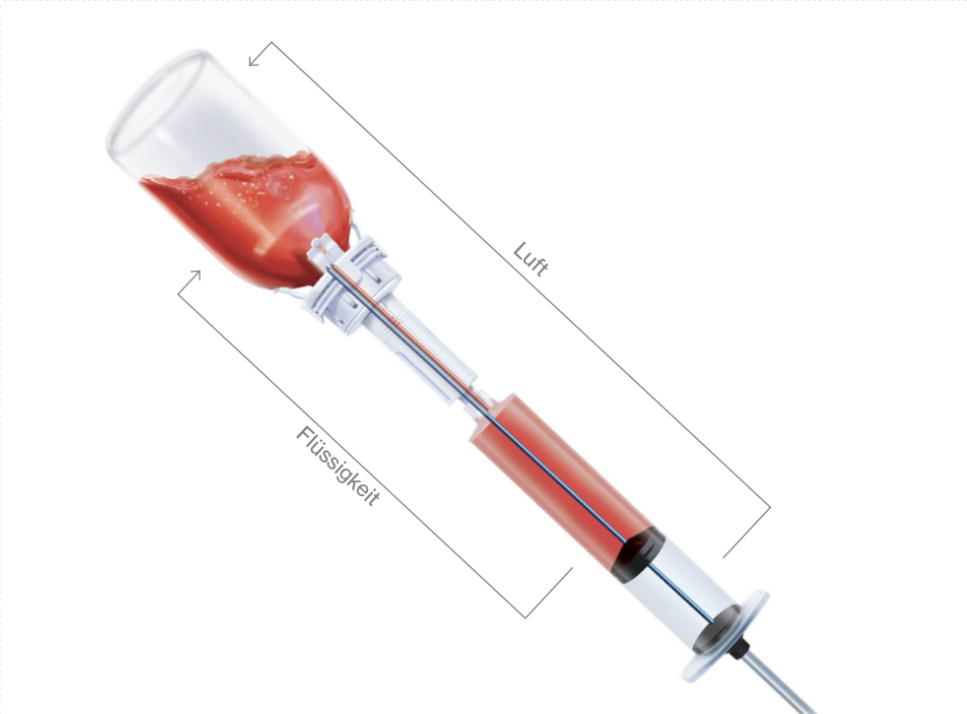
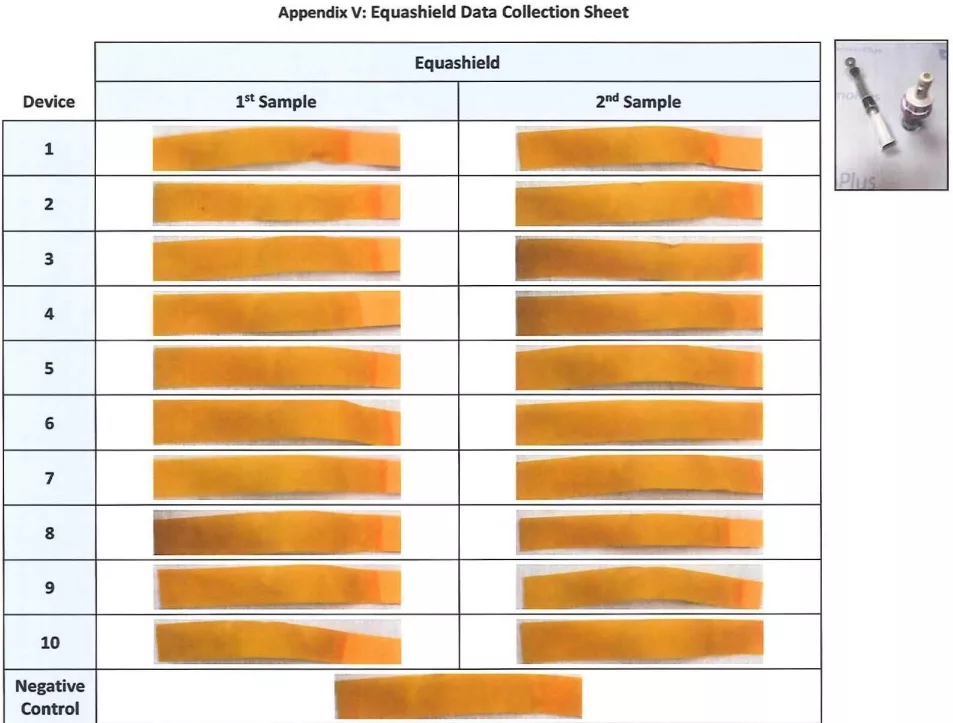
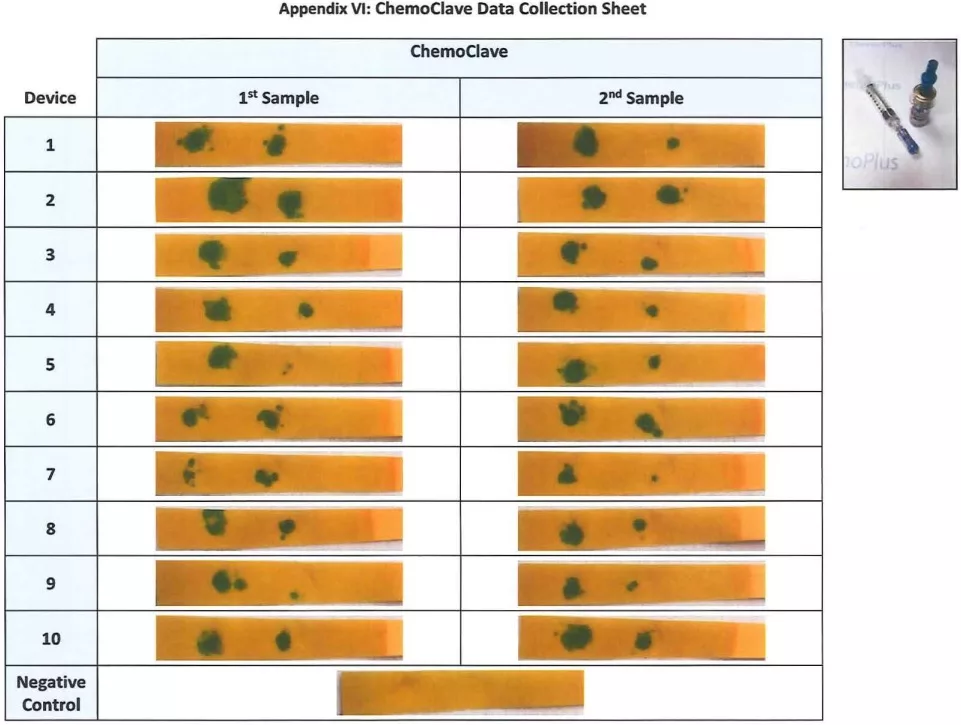
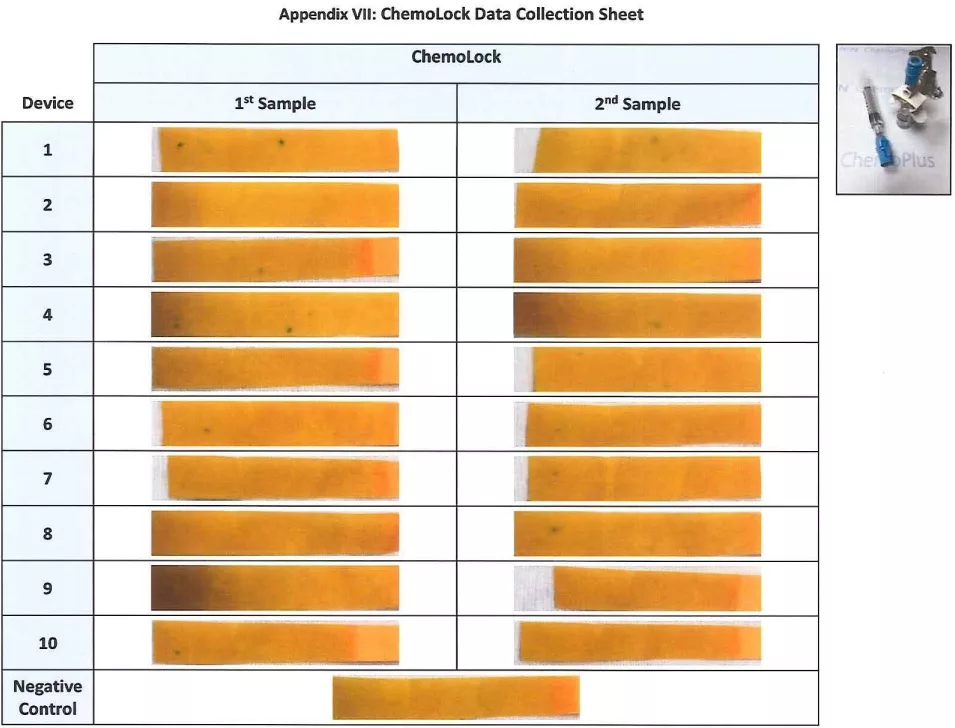
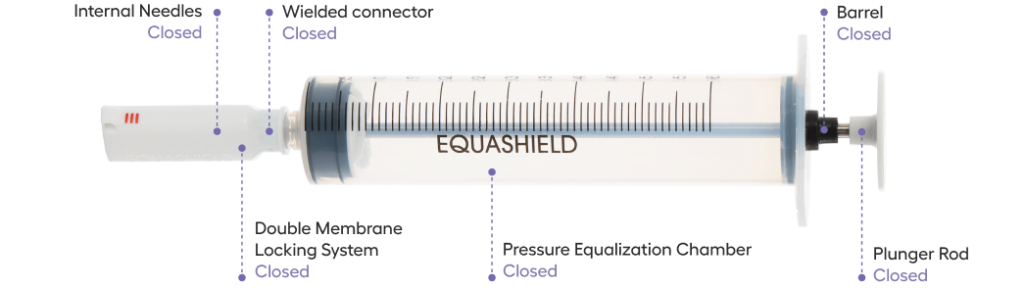
According to NIOSH, a Closed System Drug-Transfer Device (CSTD) is a device designed to mechanically prevent environmental contaminants from entering the system while also ensuring that hazardous drugs or vapors cannot escape. CSTDs allow safe preparation and administration of hazardous drugs, reducing the risk of exposure for oncology nurses. EQUASHIELD® offers CSTDs that are easy to use, efficient, and proven to minimize contamination risks.
/ Prioritize Personal Safety First: Driven by their innate empathy, nurses consistently prioritize the safety and comfort of their patients, often at their own expense. By using CSTDs like EQUASHIELD®, nurses are protected from exposure to hazardous drugs. This enables nurses to focus on caregiving without constant concern for personal safety.
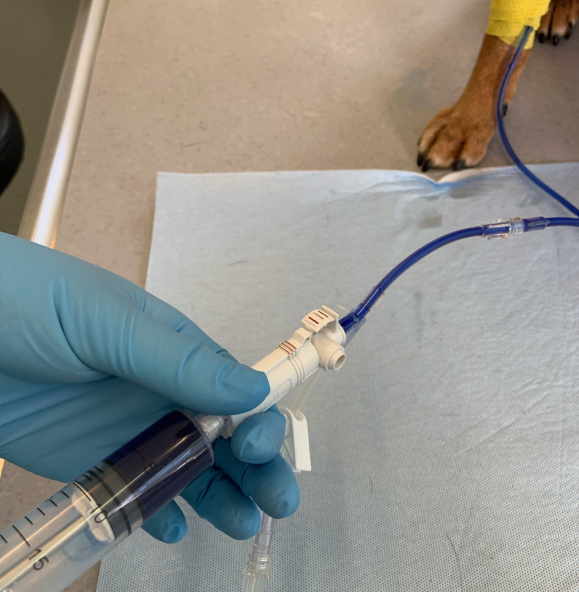
/ Secure Connections: Experience peace of mind with secure connections, guided by intuitive red-to-red markings and clicking mechanism. Designed with simplicity in mind, it reduces the stress of managing technical administrative tasks, allowing nurses to focus more on building meaningful connections with patients.
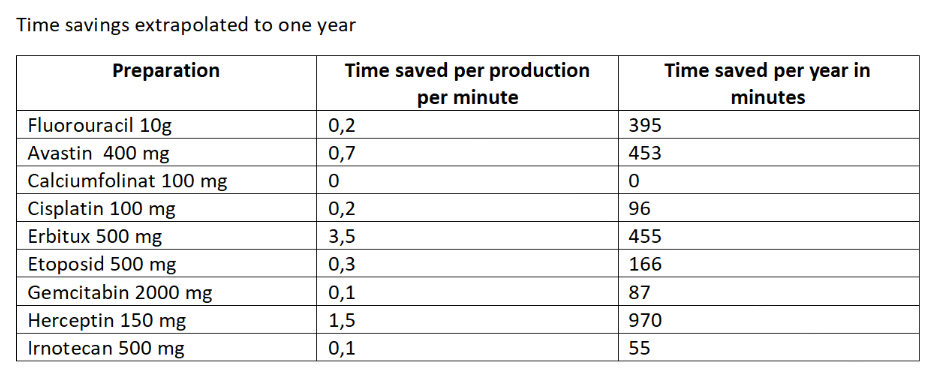
/ Streamline Workflow to Focus on Patient Connection: By spending less time on technical tasks, you can dedicate more time to building meaningful connections with your patients. Devices like EQUASHIELD®’s CSTD reduce time spent on manual tasks, freeing nurses to concentrate on providing attentive, compassionate care. EQUASHIELD streamlines the compounding process with fewer steps than any competitor and achieves the fastest average administration time in the industry.4,5
/ Ergonomic Design Means Fewer Repetitive Strain Injuries: Repetitive movements can heighten the risk of joint pain and carpal tunnel syndrome, leading to fatigue, absenteeism, and even long-term disability. These issues often contributes to job burnout, diminishing both motivation and the ability to empathize with others. EQUASHIELD CSTDs are ergonomically designed, ensuring easy handling with minimal force to handle.
Caring for Nurses to Care for Patients
For empathy to thrive in cancer care, it must be viewed as a standard—not an optional—practice. Here’s how healthcare institutions and nurses can make that shift permanent:
/ Leading By Example: Empathy must start at the top. When leadership prioritizes the health and wellbeing of the oncology staff, it sets the tone for the entire team.
/ Ongoing Guidance and Training: Implementing structured guidance and training in areas like patient communication and stress management helps nurses feel supported in their roles.
/ Building a Supportive Culture: Healthcare organizations must proactively address compassion fatigue by fostering environments where nurses can debrief, seek mental health support, and recharge.
/ Patient-Centered Policies: Advocate for systems that prioritize time for patient interactions.
/ Technology Integration: Use tools like EQUASHIELD CSTDs to streamline repetitive processes, freeing up nurses to focus on the patients.
When oncology nurses are empowered to protect their well-being, they’re better equipped to care for their patients and continue making a profound difference.
Empathy as a Transformational Tool
Empathy can transform cancer care. For oncology nurses, it drives patient-centered actions and boosts morale.
By strategically channeling empathy, oncology nurses can enhance care environments while protecting their own emotional and physical health. EQUASHIELD® recognizes the vital role nurses and pharmacists play in cancer care and is committed to developing solutions that support oncology healthcare workers.
Curious to learn how EQUASHIELD®’s Closed System Transfer Devices can elevate your practice and keep you safe? Contact us to explore your options. Let’s work together to create safer environments—for your patients and for you.