Contamination on Inner Walls of Syringes Used for Compounding and Administration of Hazardous Drugs

Abstract Introduction:
To evaluate contamination on inner walls of barrel syringes used for preparation and administration of hazardous drugs by means of wipe sampling.
Purpose
The aim of the study was to measure contamination on inner walls of syringes used for compounding hazardous drugs. As the syringes have an open connection to the environment, evaporation of the drugs could result in environmental contamination and potential exposure of healthcare workers.
Methods
Forty-three 50 mL BD Plastipak luer lock syringes were collected after single use in compounding hazardous drugs. The inner wall of the barrel was wiped for each syringe. Potential remaining contamination was also measured by liquid extraction to verify the effectiveness of the wiping procedure. Six hazardous drugs were tested. Liquid chromatog-raphy tandem mass spectrometry was used for the analysis of cyclophosphamide, doxorubicin, 5-fluorouracil, ifosfamide, and methotrexate. Platinum analysis of cisplatin was performed with voltammetry.
Results
Contamination was found for all cyclophosphamide, doxorubicin, ifosfamide, and methotrexate syringes, for eight out of ten 5-fluorouracil syringes, and for none of the cisplatin syringes. Contamination as part of the dose transferred differs between the drugs showing the highest contamination for doxorubicin (median 21.90 ppm) followed by cyclophosphamide (median 1.24 ppm), and ifosfamide (median 0.60 ppm). The lowest contamination was measured for 5-fluorouracil (median 0.02 ppm) and methotrexate (median 0.006 ppm).
Conclusion
Contamination was found on almost all syringes and differs between the drugs indicating some drugs stick more to the inner walls and plunger shafts than others. Contamination implies a potential exposure risk as hazardous drugs could evaporate from the open syringes, contaminate the working environment, and expose healthcare workers.
Introduction
When a syringe is filled with a hazardous drug (HD) during the compounding process, the inner wall of the syringe barrel is in contact with the drug that may react and stick to the surface. After transferring the HD to an infusion bag or pump reservoir, or after administration as a bolus injection, an open connection is created between the inner wall of the syringe barrel and the environment. Consequently, HDs may evaporate and potentially contaminate the working environment. Furthermore, the syringe plunger may get contaminated by contact with the inner wall of the syringe. The drug may also be transferred to the plunger during manipulation of the syringe. This may even increase if the syringe is used for multiple manipulations as observed in daily practices for instance if the volume for compounding exceeds the maximum volume of the syringe. Even during batch and dose-banding production, it is common to reuse syringes several times. The contamination on the plunger could finally be transferred via gloves of the pharmacy staff, nurse and other healthcare workers to other surfaces resulting in spread of contamination into the working environment and potential exposure of the workers. Obviously, this should be prevented as much as possible.
Even after compounding and administration, when the syringes are disposed, the evaporation process will continue resulting in contamination in and around the HD waste bin. If the syringes are not properly disposed (thoroughly wrapped or sealed), staff involved in transport and waste handling could be exposed.
Contamination on syringes used during drug compounding has been investigated previously but studies were mainly focused on contamination on the plungers. In 2005, Favier et al. detected cyclophosphamide on the plungers of all Becton Dickinson® syringes tested.1 In 2010, Kiffmeyer, repeated the study for Becton Dickinson®, Terumo®, and Equashield® syringes.2 Two, four or eight manipulations were performed for each syringe. The highest cyclophosphamide contamination was found on the plungers of the Becton Dickinson® syringes. In a separate test, cyclophosphamide was also detected on the inner walls of almost all Becton Dickinson® and Terumo® syringes. In 2014, Smith et al. performed a comparable study and compared syringe plunger contamination between Becton Dickinson® and Equashield® syringes.3 Two, four or eight manipulations were performed for each syringe.
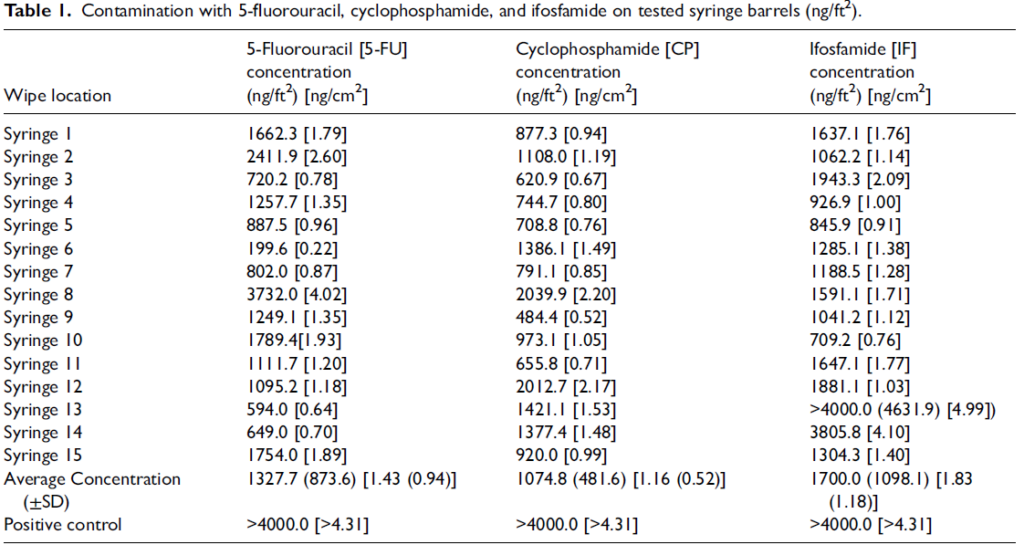
A significant higher cyclophosphamide contamination was found for the Becton Dickinson® syringes compared to the Equashield® syringes. However, execution and outcome of the study were questioned and debated as the study would not reflect routine compounding conditions (multiple manipulations), statistical analysis was flawed, controls were lacking, and sample sizes were different.4–6 Recently, Barta et al. quantified HD contamination on the inner walls of standard open barrel syringes connected to the Becton, Dickinson and Company PhaSeal® Closed System drug Transfer Device (CSTD). Single manipulations were performed for fifteen syringes 5-fluorouracil, cyclophosphamide, and ifosfamide. The inner walls of all forty-five syringes were contaminated after transfer of the drug from vial to syringe to IV bag.7 In conclusion, all studies show HD contamination on plungers and inner walls of open barrel syringes after compounding indicating a potential risk for environmental contamination and exposure of healthcare workers.
The aim of our study was to evaluate contamination on inner walls of syringes used for single use compounding of HDs by means of wipe sampling and to test for more HDs. Syringes for single use compounding or manipulation are considered as daily practice. Cyclophosphamide, ifosfamide, 5-fluorouracil, doxorubicin, methotrexate, and cis-platin syringes were selected representing HDs with different physical and chemical properties such as concentration, volatility, viscosity, and affinity to syringe surfaces.
Materials and methods
The study was performed by Exposure Control Sweden AB (Bohus-Björkö, Sweden).
HD syringes tested
Forty-three 50 mL BD Plastipak luer lock syringes were collected at the pharmacy department of the University Hospitals Leuven in Belgium (Table 1). The syringes are open barrel syringes frequently used for HD compounding. The syringes were collected after single use preparation of HDs. The drugs were transferred from the vials via the syringes to the infusion bags using the ChemoClave and Spiros CSTD (ICU Medical, San Clemente, USA). Drug volumes transferred varied from 36 to 60 mL. Fourteen operators (pharmacists and pharmacy technicians) were involved in the preparation of the syringes.
Touching the plunger shafts was not allowed to avoid contamination on the inner walls of the syringes caused by the gloves of the operators during compounding. Only the external knob on the end of the plunger was used for holding. To ascertain that the plunger shaft was not touched, the wipe samples were also analysed for nine other HDs in addition to the drug handled and transferred, except for cisplatin as the sample clean up procedure and the analysis was different compared to the other five HDs tested. In this way, potential transfer of contamination by the gloves of the operators to the prepared syringes could be established.
Six HDs were tested because physical and chemical properties of drugs differ, and this could produce different results. Only 50 mL syringes were collected for testing to allow convenient access with the wipes. Considering the 50 mL requirement, the following HDs fitted into the study: 5-fluorouracil (50 mg/mL), cyclophosphamide (20 mg/mL), ifosfamide (40 mg/mL), methotrexate (100 mg/mL), doxorubicin (2 mg/mL), and cisplatin (1 mg/mL). Two till ten syringes of each HD were collected depending on the availability of the syringes during the collection period.
After drug transfer, the syringes were individually packed and sealed in a plastic mini bag. The syringes were still connected to the Spiros CSTD to avoid spills with the HDs. Each syringe was provided with a unique code and details were registered (Table 1). The syringes were stored at 2–8°C until wipe sampling, sample preparation and analysis at Exposure Control Sweden AB.
Wipe sampling procedure
Cyto Wipe Kits from Exposure Control Sweden AB were used for surface wipe sampling (www.exposurecontrol. net). To perform a proper sampling, the original wipe (45 cm×24 cm) was rolled into a cylinder-shaped wipe of 12 cm in length and about 1 cm in diameter enabling easy entering the barrel (Figure 1). The plunger was set at 10 mL to have sufficient access into the syringe barrel to be able to take the wipe sample and to avoid touching of the plunger shaft. Consequently, the inner wall between 0 and 10 mL was not wiped. After the wipe was positioned in the barrel, the syringe was positioned upright, and 5 ml 0.1% formic acid solution or 5 ml 0.5 M HCL solution (for cisplatin) was dripped on the wipe. Next, the plunger was turned around to make sure the prewetted wipe contacted the total surface of the inner wall of the syringe.
The prewetted wipes were collected and extracted with 20 mL 0.1% formic acid solution. For cisplatin 20 ml 0.5 M HCL solution was used. Total extraction volume for the wipe samples was 25 mL. After extraction, a part of the extract was used for analysis.
The remaining contamination on the inner walls of the syringes was also measured after wiping to verify the effectiveness of the wiping procedure. Thereto, the syringes were placed upright with the plunger still set at 10 mL, and 50 mL 0.1% formic acid solution was poured in the space between barrel and plunger.2 For the cisplatin syringes, 50 ml 0.5 M HCL solution was used. The liquids were removed after 60–90 min and analysed separately from the wipe samples.
The wipe samples and liquids were also analysed for nine other drugs in addition to the drug handled and transferred, except for cisplatin as the sample clean up procedure and the analysis was different compared to the other five drugs tested.
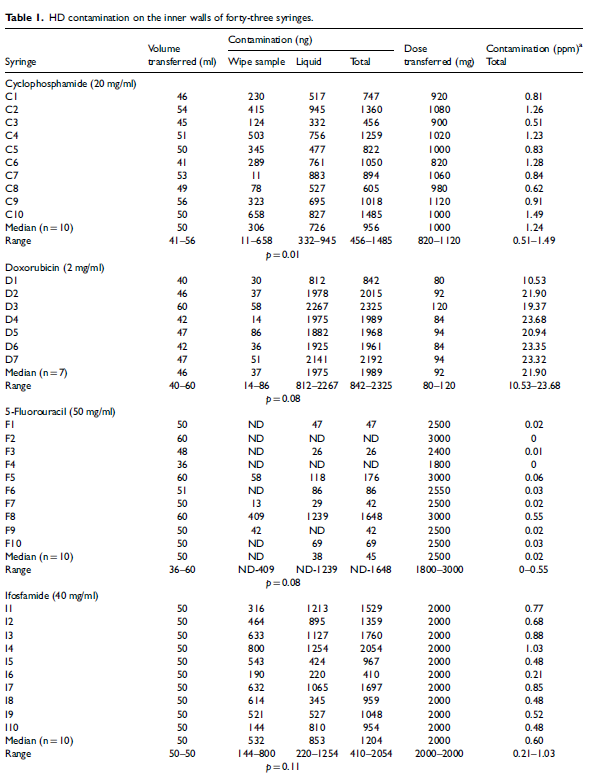
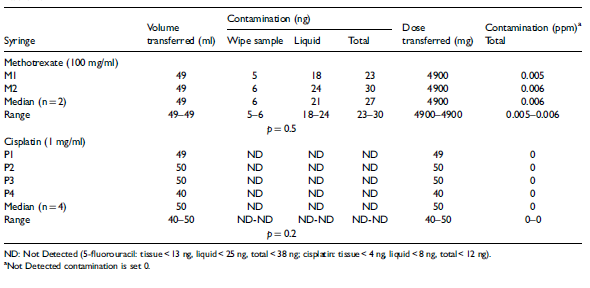
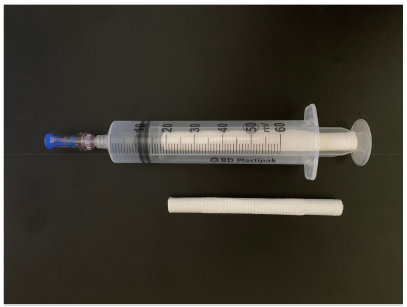
Figure 1. Cylinder-shaped wipe and syringe with cylinder-shaped wipe inside the barrel
Liquid chromatography with tandem mass
spectrometry analysis
Liquid chromatography with tandem mass spectrometry (LC-MS/MS) was used for the analysis of cyclophosphamide, doxorubicin, 5-fluorouracil, ifosfamide, methotrexate, and the other five HDs not handled and transferred but measured to check for potential (cross)contamination on the plunger shaft (cytarabine, docetaxel, etoposide, gemcitabine, and paclitaxel). Details of the analytical method and equipment used have recently been published.8 The detection limit is 0.01 ng/mL for cyclophosphamide, cytarabine, gemcitabine, ifosfamide and methotrexate, 0.2 ng/mL for docetaxel, doxorubicin and paclitaxel, and 0.5 ng/mL for etoposide and 5-fluorouracil.
Stripping voltametric analysis
Platinum analysis of cisplatin was performed with stripping voltammetry.9 0.5 mL of the extract was destructed using hydrogen peroxide, hydrochloric acid and UV-light resulting in the formation of platinum ions. Finally, the platinum ions were analysed instead of cisplatin. Samples were analysed in duplicate including destruction step. Mean values are reported. Due to background levels of platinum, the limit of quantification is set at 0.1 ng/mL. This corresponds to 0.16 ng/mL cisplatin.
Statistical analysis
All analyses were performed in R (version 4.4.1) using the R package rstatix (version 0.7.2) for statistical tests and ggplot2 (version 3.5.1) for visualisation. Wilcoxon’s non-parametric test was used for comparison of the contamination between wipe samples and liquids for each of the HDs (Table 1). Total contamination in the syringes as part of the total amount of HD transferred and presented in ppm, was also compared between the six HDs using Wilcoxon’s test. p values were adjusted for multiple com-parison using the Holm’s method. For values below the detection limit, half of the detection limit was used. p values below 0.05 were considered as significant different.
Results
Contamination measured by wipe sampling was found on the inner walls of all cyclophosphamide, doxorubicin, ifosfamide and methotrexate syringes (Table 1). 5-Fluorouracil was detected on the inner walls of four out of ten syringes. Contamination with platinum, representing cisplatin, was not detected on the four syringes tested. Comparable results were found for the remaining contamination measured in the liquids, to verify the effectiveness of the wipe sampling procedure. Contamination was again found for all cyclophosphamide, doxorubicin, ifosfamide, and methotrexate syringes, for seven out of ten 5-fluorouracil syringes, and for none of the cisplatin syringes (Table 1).
The highest total contamination (wipe samples and liquids) was measured for doxorubicin (median 1989 ng), followed by ifosfamide (median 1204 ng), and cyclophosphamide (median 956 ng). The lowest contamination was measured for 5-fluorouracil (median 45 ng) and methotrexate (median 27 ng). Cisplatin was not detected.
For cyclophosphamide, contamination was higher in the liquids than in the wipe samples (p = 0.01), while no differences were found for the other HDs. This indicates that the wipe sampling on the inner walls was not effective. Effective wipe sampling would have resulted in higher wipe sample contamination than liquid contamination.
Contamination on the syringes with the nine other HDs, apart from the HD compounded, to check for potential transfer of contamination by the gloves of the operators, was not found for the wipe samples and the liquids indicating no HD cross contamination during collection of the syringes and sampling in the laboratory.
To compare the contamination between the six HDs, the total HD dose transferred must be calculated for each of the syringes by multiplying the HD concentration with the volume transferred. Next, the contamination as part of the total amount of HD dose transferred is calculated and is expressed in parts per million (Table 1). Median values and ranges are presented and used for statistical analysis. The highest total contamination is calculated for doxorubicin (median 21.90 ppm), followed by cyclophosphamide (median 1.24 ppm), and ifosfamide (median 0.60 ppm). The lowest total contamination is calculated for 5-fluorour-acil (median 0.02 ppm) and methotrexate (median 0.006 ppm). Significant higher contamination was found for doxorubicin compared to cyclophosphamide, ifosfamide, and 5-fluorouracil (p = 0.001), and for cyclophosphamide (p = 0.0003), and ifosfamide (p = 0.002), compared to 5-fluorouracil.
Discussion
The aim of the study was to measure contamination on inner walls of syringes by means of wipe sampling. Contamination was found on all doxorubicin, methotrexate, cyclophosphamide and ifosfamide syringes. A few 5-fluorouracil syringes were also contaminated but none of the cis-platin syringes. Although the focus was to wipe the inner walls of the syringes, it cannot be excluded that the contamination measured also includes contamination on the plunger shaft.
The effectiveness of the wipe sampling procedure was validated by measuring the remaining contamination on the inner walls of the syringes after wiping. Thereto, a liquid was poured into the barrel enabling the remaining drug to dissolve. However, the results show higher amounts of drugs in the liquids than in the wipe samples, except for the cisplatin syringes where no contamination was found. This indicates that the wipe sampling procedure was less effective than the use of the liquid. In addition, contamination could also be present on the plunger shafts. As the wipes also touch the plunger shafts, contamination on the plunger shafts will be sampled too. This also concerns sampling with the liquids.
Each syringe (except for cisplatin) was also checked for contamination with nine other drugs to measure potential transfer of contamination by the gloves of the operators to the plunger shafts. No other drugs were detected except the ones compounded. This indicates that it is very unlikely that the measured contamination on the inner walls and plunger shafts of the syringes is caused by other (previous) activities than the compounding itself. It also shows that the syringes were properly collected and that the wipe testing and the collection of the liquids at the laboratory was performed without contamination.
It should be noticed that the inner walls of the syringes were not wiped between 0 and 10 mL as the plunger was set at 10 mL to perform the wipe sampling. This indicates an underestimation of the contamination with about 20 percent based on the volume transferred (median 50 mL; range 36–60 mL).
The results were not corrected for recovery, and it remains unclear if all drugs were removed by the wipes or were present in the liquid. Laboratory test performed in duplicate give some indication and show high recoveries for cyclophosphamide (96%) and ifosfamide (92%), moderate recoveries for cisplatin (80%), methotrexate (69%) and 5-fluorouracil (62%), and low recoveries for doxorubicin (19%). This indicates that some drugs stick more to the inner walls of the syringes than others especially doxorubicin. Differences can be explained by different product characteristics such as physical and chemical properties of the drugs.
The main limitation of the study concerns the ineffective wipe sampling, but this was compensated by the additional extraction of HDs on the inner walls and plunger shafts. In addition, it remains unknown whether, and how much of each HD will evaporate from the inside of the syringes and will finally be transferred as contamination into the environment.
Some (parts of the) drugs might permanently stick on the inner walls and plunger shafts of the syringes and will not be released into the environment. Despite these uncertainties, the total amount of HD contamination on the inner walls and plunger shafts of the syringes is relevant as they indicate a potential risk for environmental contamination and exposure of healthcare workers. Evaporation of HDs has been proven at room temperature in addition to release of HD particles during com-pounding.12–16
Considering the hierarchy of controls to protect workers from exposure to HDs, the focus must be on engineering controls (level 3) to isolate workers from the HDs as elimination (level 1: remove the HDs) and substitution (level 2: replace the HDs) are impossible.10,11 Patients need HDs for treatment. Administrative controls (level 4) and finally PPE (level 5) are the next steps but considered as the least effective in protection of healthcare workers. Engineering control measures, to minimise the potential spread of contamination from the inner walls and plunger shafts of the syringes to the environment, could include:
/ Single use compounding of the syringes (draw and push once).
/ Wrap or seal the syringes immediately after use. This includes transfer from vials in bags and pump reservoirs during compounding and after administration to patients.
/ Make sure the syringes are properly wrapped or sealed when discarded in a hazardous waste bin, to avoid contamination by vapours and particles from HD waste.
/ Do not use open barrel syringes but sealed syringes. Following these recommendations could result in reduction of environmental contamination and potential exposure of the operators and nurses.
Following these recommendations could result in reduction of environmental contamination and potential exposure of the operators and nurses.
Conclusion
This study has shown that routine HD compounding has resulted in contamination on the inner walls and plunger shafts of syringes for five out of six HDs tested. Some HDs stick more to the inner walls and plunger shafts than others resulting in differences in contamination between the HDs. However, most important is that the contamination on the inner walls and plunger shafts of the syringes could result in release of the drugs into the working environment and exposure of the healthcare workers. This phenomenon should be considered in taking risk management measures when handling HDs.
Acknowledgements
Statistical support from Björn Andersson and Jari Martikainen (Statisticians at the Bioinformatics and Data Centre at the Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden), is kindly acknowledged.
Author contributions
All authors designed the study; PS and BT, collected the data; PS, performed the analysis and interpreted the results; PS, drafted the manuscript. All authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for the research and writing this publication was provided by Equashield Medical Ltd, Migdal Tefen, Israel.
ORCID iD
Paul Sessink https://orcid.org/0000-0002-8580-0044