Introduction
Our institution administers thousands of monthly chemotherapy doses, so we were very early adopters of both USP7971 and NIOSH recommendations. 2 We had developed and implemented policies and procedures outlining safe and appropriate procedures for handling oncological agents, the utilization of cleanrooms and biological safety cabinets, personal protective equipment (PPE), and many other protective measures. Those policies and procedures included the utilization of the Phaseal Closed System Transfer Devices (CSTD) with Becton Dickinson (BD) syringes. Three years ago, we replaced the Phaseal devices with a new CSTD, Equashield. The design, simplicity, ergonomics, and the potential for decreasing our hazardous waste we felt offered an advantage over the BD Phaseal products. Favier et al.,3 in a peer-reviewed study, examined the potential for syringe plunger contamination during routine drug preparations at hospital pharmacies. This study confirmed and quantitated that considerable contamination from cyclophosphamide did occur on the BD syringe plungers. This study included wipe test sampling of syringe plungers from syringes that were purposely operated with repeated withdrawal and re-injection cycles of cyclophosphamide to simulate repeated use. The study also performed wipe test sampling of syringes collected after normal use during a pharmacy routine work day. Both groups of syringe samples were found to be contaminated. This previously undetected route of exposure poses a problem as it has identified another potential source of contamination of gloves and the work environment, which increases the risk of exposure to the pharmacy staff, nurses, patients, and their families. These findings highlight the urgent need for improved safety measures in healthcare settings. An essay on nursing should address this issue, emphasizing the importance of proper handling and disposal of hazardous substances to protect both healthcare professionals and patients. A few years later, a research laboratory specializing in antineoplastic agents and environmental contamination repeated the plunger contamination study.4 This study included Equashield syringes in addition to BD and Terumo syringes. This study confirmed the findings of the previous study3 with high contamination rates of up to 0.5 mg cyclophosphamide found on both the BD and Terumo syringe plungers. Since both manufacturers, BD and Equashield have claimed to have made enhancements in the performance of their products, we asked Equashield to sponsor a similar comparative study at our institution. Equashield agreed and a small study was developed that would test the levels of contamination of the BD syringes with Phaseal CSTD devices against those from Equashield.
Karmanos Cancer Center, Detroit, MI, USA
Corresponding author:
Stephen T Smith, Department of Pharmacy, Karmanos Cancer Center,
4100 John R. Street, Mailcode: WE01PH, Detroit, MI 48201, USA.
Email: [email protected]
Method
The study included 11 Equashield 60 mL syringe units and 12 BD PlasticTM 60 mL syringes. The Equashield syringes are a stand-alone closed system that includes factory built-in closed pressure equalization system and dry connectors. The BD syringe is a traditional single use syringe with a luer lock tip manually attached to the appropriate Phaseal dry connector (Injector). The closed pressure equalization system is built-in the Phaseal vial adapter (Protector).
The difference between the BD and the Equashield syringes is shown in Figures 1 and 2. The BD syringes have an open syringe barrel and a regular four ribs plunger structure. The Equashield barrel is sealed by a lid and the plunger is a small diameter metal rod that can move through the lid. A seal, seated in the center of the lid, seals the rod and ensures airtight operation of the syringe.
Four Equashield Vial Adaptors (VA-20) and four Phaseal Protectors (P-50) were attached to eight cyclophosphamide 2 g vials, respectively. Each vial was reconstituted with 100 mL of standard sodium chloride 0.9% solution to a final concentration of 20 mg/mL. There were eight syringes and adaptors utilized of each system to complete the transfer in 50 mL aliquots into the drug vials.
The syringes were divided into three equal groups for the Equashield and BD syringes, with a vial of the reconstituted cyclophosphamide designated for each group with the exception of the last group which received 2 vials each. A 50 mL aliquot of cyclophosphamide was drawn into each syringe and then injected back into the cyclophosphamide vial. This drug transfer procedure was immediately repeated twice for the syringes in group 1, four times for the syringes in group 2, and eight times for the syringes in group 3. Only 50 mL were drawn into the syringes to remain within the manufacturers’ guidelines of use and minimize the potential for a possible spill. The same withdraw and reinjection processes were applied to the syringes which were similar to those one would encounter during a routine pharmacy compounding procedure.
After the completion of the drug transfers with the Equashield and BD Phaseal syringes, the plungers were retracted back to the nominal syringe marking and a wipe test of the exposed plunger was done.
A wipe sample was taken from the biological safety cabinet work surface at the commencement of the study to rule out any possible contamination prior to the study. The size of the wiped surface was 1 ft2 (930 cm2).
The services of ChemoGloTM (Chapel Hill, North Carolina), a specialized third-party laboratory, were used to accurately quantify trace amounts of cyclophosphamide on the syringe plungers and work area sample. The ChemoGloTM assay has a low detection level of 10 ng (1 109 ) per wipe sample and is simple to use. The assay is optimized for wipe sampling of any surface area up to 1 ft2 (930 cm2), which is optimal for wiping the smaller surface of the syringe plungers. The quantification of cyclophosphamide is, therefore, the total quantity of cyclophosphamide in nanograms found on a plunger/wipe sample.
Four kits were utilized for a total of 24 wipe samples (each kit consisting of six wipes samples) which were completed in accordance to the procedures outlined by ChemoGloTM.
The wipe samples were taken using the ChemoGloTM swab with absorbed solution. The plungers were retracted back to the nominal syringe marking and the exposed plungers wiped thoroughly with the wet swabs. After the completion of the wipe sampling, the swab was placed in a dedicated labeled container. Since each wipe sample consists of two swabs and solution containers, this process was repeated for the secondary swab sampling.
All 48 containers with the wipe samples (two containers for each syringe 23 syringes, and two containers for testing the work surface) were sent overnight to ChemoGloTM laboratory for the performance of sample extraction and analysis with LC-MS/MS technology.
The test was performed in a Thermo Class II, A2 Biological Safety Cabinet by an experienced chemotherapy-certified pharmacy technician, proficient with the use of both the Equashield and Phaseal CSTDs. The working area was cleaned in accordance to our facility’s standard procedure prior to initiation of the study. To isolate the study and exclude any foreign source of contamination that may influence the results, the drug vials were cleaned with IPA pads and only materials which are required for the study were kept in the hood. Large absorbent pads were used to cover the whole work area. The pads were replaced and the gloves changed before working with each group of syringes.
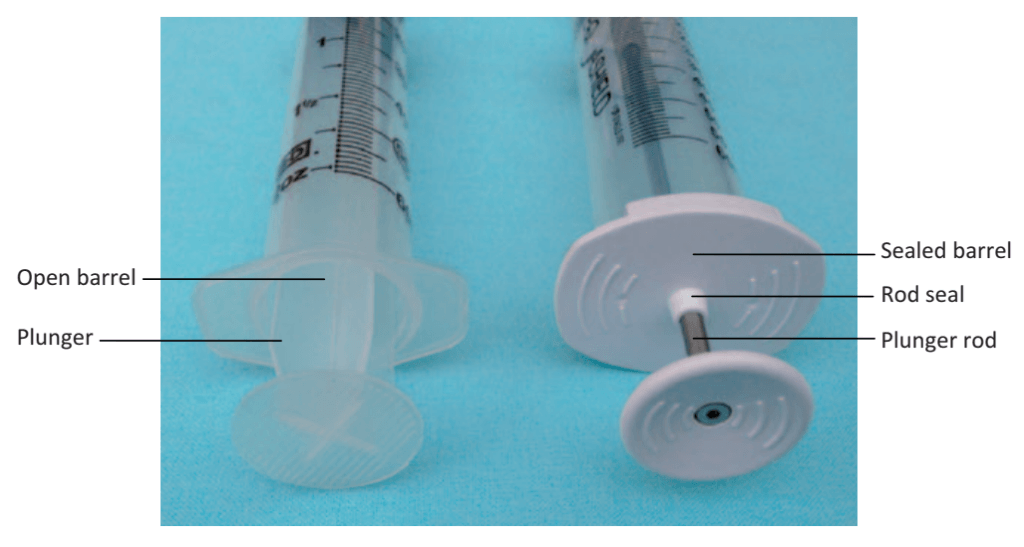
Figure 1. The BDÕ syringe (left) and the EquashieldÕ syringe (right).
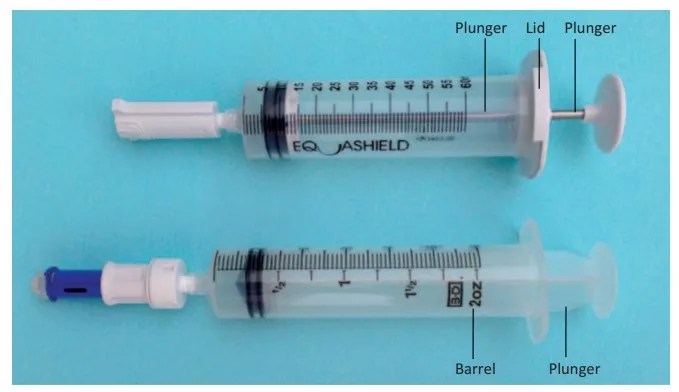
Figure 2. The EquashieldÕ syringe (top) and the BDÕ syringe (bottom).
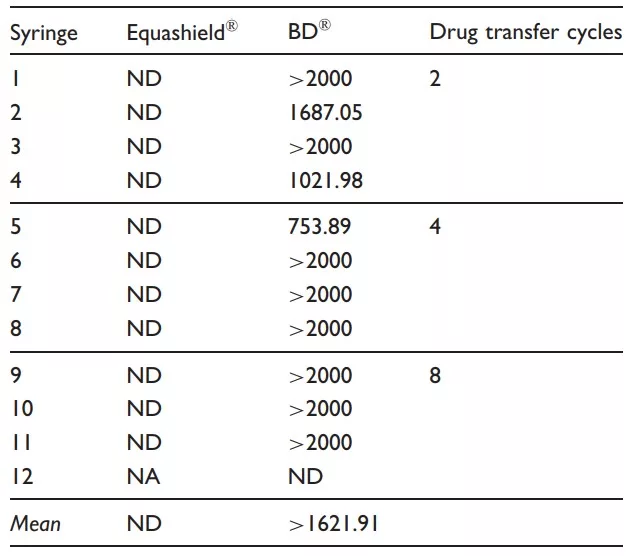
Table 1. Amounts (ng) of cyclophosphamide on the tested syringe plungers.
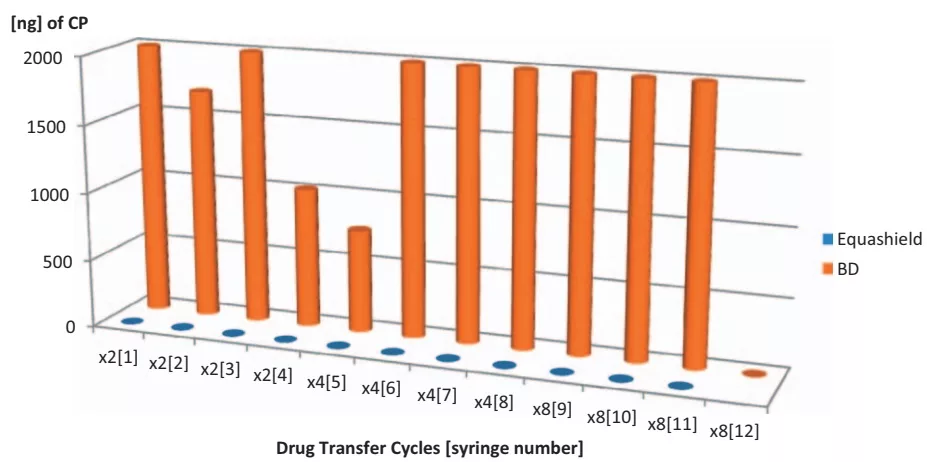
Figure 3. Contamination levels (ng) of cyclophosphamide (CP) on the tested syringe plungers.
Results
Results demonstrated significant cyclophosphamide contamination levels on 11 out of 12 BD syringes, whereas all 11 Equashield CSTDs had undetectable concentrations. The 1 ft2 (930 cm2 ) work area wipe showed minor contamination of 16.82 ng, considered to be close to the lower limits of detection level (LLQ) (Table 1).
Statistical assessment
We regard this study to be a small-scale pilot study with the intent of reviewing the two CSTDs that we were familiar with. We had little preliminary data to determine the study’s sample size; therefore, an assumption of 11 syringes was made based on previous studies.3,4 The results confirmed the assumption and show that the average contamination level for the BD plungers was ¼ 1622 ng with a variant, 2 ¼ 331 ng2 . Assuming a normal distribution, CP ~ N(µ, σ2 ), the average contamination level on the BD plunger was greater than 1228 ng, with a confidence level of 95%. That is to say, that if we used an unlimited number of syringes, we could be 95% sure that the averaged contamination level would be above 1228 ng. Since the technology is limited to detect and quantify between 10 ng and 2000 ng, for the statistical analysis of the results, we assumed that when the contamination was above the technology’s detection limit, we regarded it to be 2000 ng understanding that the true level of contamination may exceed that value several-fold. This has already been documented in previous studies 4,5 using HPLC-MS/MS analysis method (Figure 3).
The lower limits of detection (LLQ) for these assays are 10 ng. Quantities that are less than the LLQ are defined as non-detectable (ND). The upper limits of detection for these assays are 2000 ng. Quantities that are greater than 2000 ng are defined as > 2000.
Discussion
The contamination levels found on the standard BD syringe plungers confirm previous studies.3,4 This contamination highlights the potential of a significant source of low-level exposure for healthcare workers
while they prepare and handle hazardous drugs during their routine workday. It is suggested that the staff’s gloves come into contact with the syringe’s contaminated plungers then in turn, touch other surfaces such as the work area, the prepared IV bags which are distributed to patient care areas, and so forth, thus contaminating the entire work environment and increasing the potential of exposure.
Following the results of previous study,4 where contamination was also found on tested Terumo syringes, it is most likely that BD syringes generally represent standard syringes of other manufacturers as well.
Furthermore, the contamination on standard plungers is expected regardless of use of a CSTD or traditional methods when handling hazardous drugs.
Similarly, our results demonstrated no detectable level of contamination on the Equashield syringe plungers which supports previous findings3,4 as well as the NIOSH recommendations2 that endorse the use of CSTD which mechanically prohibits the escape of hazardous drug or vapor concentrations outside the system in order to minimize exposure to hazardous drugs.6
We believe that cyclophosphamide infiltrates on to the plungers of standard BD syringes by reacting and creating a layer on the inner walls of the syringe barrel.
The very minimal distance or direct contact between the plungers to the contaminated walls ‘‘allows’’ cyclophosphamide to ease its way on to the plunger. The typical squeezing of the barrel, bending or twisting of the plunger during real use conditions often creates a direct contact between plungers to the contaminated walls, thereby allowing transfer of contamination. It has been shown that the safety measures adopted through the Equashield design address the risk of plunger contamination7 by preventing contact and ensuring greater distance between the Equashield plunger rod and the syringe barrel in this contained CSTD.
Finally, the contamination levels of cyclophosphamide found on the work area sample were close to the LLQ and may therefore be considered of little consequence.
Conclusions
This study has confirmed the hazards associated with standard syringes and the importance of using appropriate closed system syringes during all preparation and handling stages of hazardous drugs, in order to significantly reduce healthcare workers’ exposure to contaminated surfaces and work environments. It is suggested that in light of this study, and the medical literature which it echoes, further investigation and consideration are required, and more rigorous regulations and policies should be established in this area in order to further minimize risks and optimize the safety of healthcare workers.
Funding
This study was partially sponsored by Equashield.
Conflict of interest
The authors have no conflict of interest to disclose.