Introduction
Exposure to cytotoxic medicines poses a significant health risk to healthcare workers who prepare and administer chemotherapy.¹ Occupational exposure is possible for all hospital staff, but pharmacy staff preparing doses of cytotoxic medicines are at increased risk. To minimise exposure, staff must wear personal protection equipment and prepare cytotoxic medicines in a cytotoxic drug safety cabinet (CyDSC) or isolator, housed within a cleanroom.¹⁻⁶
Workplace Health and Safety Queensland and the American National Institute for Occupational Safety and Health (NIOSH) recommend healthcare workers use a closed-system transfer device (CSTD) during the handling of cytotoxic medicines to minimise the risk of occupational exposure.¹˒⁴ A CSTD is defined as a drug system transfer device that mechanically prohibits the transfer of environmental contaminants into the system and the escape of hazardous medicine or vapour concentrations outside the system.⁴ As CSTDs have different design concepts, such as physical-barrier versus air-cleaning technology, it can be difficult to compare performance.
NIOSH is developing an independent testing method for CSTD performance and draft a performance test protocol for CSTDs used during pharmacy compounding and administration of hazardous drugs was published in 2016.⁷˒⁸ Using the draft NIOSH test protocol, Wilkinson et al., Halloush et al., and Forshay et al., independently tested a variety of commercially available CSTDs such as Equashield (Equashield Compounding Technologies, Port Washington, NY, USA), Tevadaptor (Simplivia Healthcare Ltd., Hod Hasharon, Israel), PhaSeal (Becton, Dickinson and Company, Franklin Lakes, NJ, USA), ChemoClave (ICU Medical Inc., San Clemente, CA, USA), HALO (Fresenius Kabi, Bad Homburg, GER), ChemoLock (ICU Medical Inc., San Clemente, CA, USA), OnGuard (B Braun SE, Melsungen, GER), and Texium (Becton, Dickinson and Company, Franklin Lakes, NJ, USA).⁹⁻¹¹ Equashield and PhaSeal passed all NIOSH testing. The physical-barrier-type CSTDs Equashield and PhaSeal have the most evidence to be classed as a CSTD.
The local hospital pharmacy compounding unit, located in Queensland, Australia, has used PhaSeal since opening in 2014 and it had been used at the former (legacy) site since 2010. The use of PhaSeal was introduced at the original hospital site after cytotoxic contamination was detected on pharmacy checking benches, the outside of cytotoxic infusion bags, and on the oncology ward. Introduction of PhaSeal eliminated contamination, as previously reported in a number of publications.¹²⁻¹⁵
Equashield is a competitor product to PhaSeal that may be an acceptable, or possibly a superior, alternative CSTD. Massoomi tested six CSTD systems — Equashield, PhaSeal, ChemoClave, ChemoLock, VialShield (CareFusion, San Diego, CA, USA) and OnGuard with Tevadaptor — and demonstrated a failure rate of 0% for Equashield, 30% for PhaSeal, and the remaining systems had a failure rate of 85–100%.¹⁶ The PhaSeal CSTD system uses standard open-back syringes whilst the Equashield CSTD system provides a closed-back syringe unit. Smith et al. examined the contamination levels of cyclophosphamide on the syringe barrel and plunger of Becton Dickinson syringes connected to PhaSeal components, compared to the closed-back Equashield syringe unit. Significant contamination levels were detected on most of the Becton Dickinson syringe plungers compared to no contamination on the Equashield syringes.¹⁷ Nurgat et al. determined Equashield required fewer compounding steps and there was a decrease in clutter and packaging in the CyDSC, with pharmacy staff preferring Equashield to PhaSeal.¹⁸
The aim of this study was to determine if Equashield provides any advantages financially, in compounding time, rubber bung contamination, cytotoxic medicine surface contamination, staff satisfaction, and work health and safety benefits when compared to PhaSeal.
Method
Ethics Statement
This project was exempt due to the local policy requirements that constitute research by the Children’s Health Queensland Research Ethics Committee (Reference no: EX/23/QCHQ/97690). The justification for this ethics exemption was as follows: the study conformed with the National Health and Medical Research Council Ethical considerations in quality assurance and evaluation activities and met local requirements for a quality assurance activity and did not involve any assessment of staff. Informed consent was obtained from all staff via verbal explanation of the project and their voluntary participation. Staff consented via completion of the voluntary survey.
Study Design
The hospital pharmacy compounding unit completed a 4-month trial in 2019. The pharmacy compounded cytotoxic infusions with Equashield instead of PhaSeal. Chemotherapy presented in a syringe continued to be prepared using PhaSeal. All cytotoxic doses that did not use a CSTD (intrathecal, subcutaneous, and intramuscular) were excluded from the study. The trial was designed purposely to avoid changing the method of chemotherapy administration at the hospital, to avoid the need to retraining nursing staff.
The trial evaluated six key characteristics of each CSTD. These were:
- financial impact;
- compounding time;
- rates of bung contamination;
- surface cytotoxic contamination levels;
- staff satisfaction; and
- work health and safety.
Financial Impact
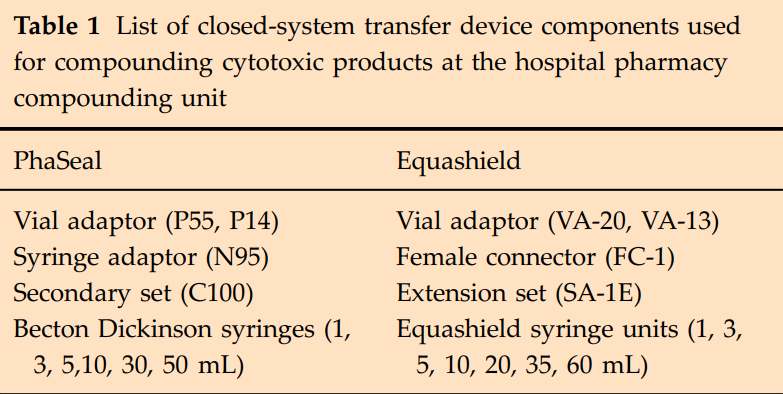
A retrospective financial analysis of 6 months of compounded products was performed. A report detailing all the cytotoxic products administered was prepared from the electronic Oncology Information Management System, Charm Health (The Citadel Group, Melbourne, Vic., AUS). Each product was evaluated by a senior compounding pharmacist to determine what CSTD components were required for the pharmacy to compound the product using PhaSeal and Equashield.
These data were entered into a spreadsheet to compare the financial difference based on the hospital contract pricing. Consideration was given to the dose, how many vials were required, and if powder reconstitution was necessary. The components for each CSTD are listed in Table 1.
The medicine cost and staff time taken to prepare, personal protective equipment, and cleanroom maintenance were not included in the financial analysis.

Compounding Time
During the trial, 21 items were prepared by the same two compounding technicians using both PhaSeal and Equashield with the time taken to compound each item recorded. The items chosen were the five most frequently compounded chemotherapy infusions (vincristine, carboplatin, doxorubicin, dexrazoxane, and etoposide phosphate). An experienced and recently trained technician compounded the items. The time taken to gown, glove, and clean the CyDSC was excluded.
Rates of Bung Contamination
During the trial, each infusion compounded using Equashield was inspected for visible particulate contaminant by two compounding trained pharmacists independently, under fluorescent light. All product contamination was noted and the dose was remade if deemed contaminated.
Surface Cytotoxic Contamination Levels
Cytotoxic surface contamination wipe sampling was performed prior to, and after the trial, at five locations (middle of the CyDSC work tray, cytotoxic cleanroom trolley, assembly bench, checking/labelling bench, and computer bench). Wipe sampling was performed as per the WorkCover New South Wales (NSW) Chemical Analysis Branch Wipe Sampling Kit directions.¹⁹ The samples were analysed by the Chemical Analysis Branch (detection limit 3 ng/sample). Cyclophosphamide, etoposide, doxorubicin, ifosfamide, methotrexate, and vincristine were chosen based on the frequency of compounding and the ability of detection by the Chemical Analysis Branch.
Staff Satisfaction
Ten consenting pharmacy compounding staff members were asked to complete a survey of 15 questions comprising 13 Likert scale and two direct comparison preference responses to determine their subjective opinion of working with each CSTD (Table 2). Seven staff had over 12 months of experience and three staff had less than 3 months of compounding experience.
The PhaSeal survey was completed prior to the introduction of Equashield. The Equashield survey was completed at the end of the 4-month trial period. Staff identified themselves on the survey to determine their experience and familiarity with compounding. Surveys were completed on paper and staff had 1 week to complete the survey on each occasion.
Work Health and Safety
The hospital Work Health and Safety (WH&S) team performed an ergonomic review of both CSTDs, including force gauge testing, visual observation of each CSTD and compounding sessions, repetitive movement, volumes of product compounded, and staff interviews.
Other Benefits or Disadvantages
A risk assessment by the hospital infection management and prevention (IMP) team was performed and any benefits or disadvantages realised while using Equashield that did not fall within the six key characteristics outlined above were recorded.
Results
Financial Impact
Compounded products included carboplatin, cisplatin, cyclophosphamide, cytarabine, daunorubicin, doxorubicin, etoposide phosphate, fludarabine, ganciclovir, gemcitabine, ifosfamide, methotrexate, mitoxantrone, pemetrexed, topotecan, vinblastine, vincristine, and vinorelbine.
The financial analysis of 1968 compounded products showed the cost of using PhaSeal was AUD $37,609. The cost to compound the same products using Equashield was AUD $42,293.
Compounding Time
The total time taken to compound 21 products using PhaSeal was 90 min. When the same infusions were compounded by the same staff members using Equashield, the total compounding time was 71 min, equating to a time saving of 19 min, approximately 1 min per product.
When comparing the experienced versus non-experienced technicians, the more experienced staff member compounded faster. To prepare a vincristine infusion the experienced compounder took, on average, 2.3 min using PhaSeal but the less experienced technician took 2.9 min. To compound the same product using Equashield, the experienced staff member took 1.75 min and the less experienced technician took 2.5 min.
The mean time in minutes to compound a product using PhaSeal was 4.3 min (range 2.2–17 min) and for Equashield was 3.4 min (range 2–10 min).
Rates of Bung Contamination
Equashield was used to compound 1839 cytotoxic infusions and three products contained rubber bung core contamination.
Surface Cytotoxic Contamination Levels
Wipe sampling prior to the study and again at the end of the trial showed no detectable levels of cytotoxic surface contamination in the pharmacy compounding unit.
Staff Satisfaction
Ten staff (six pharmacists and four pharmacy technicians) were surveyed. Seven staff had over 12 months of experience and three staff had less than 3 months of experience. The list of questions and the mean five-point survey score for each question put to the staff members are listed in Table 2.
A statistically significant difference (p < 0.05) was only recorded for three questions (compounding without contamination, using the system on smaller vials, and compounding without flooding the system).
On the direct comparison question, when staff were asked which CSTD was faster to use, all answered Equashield. Eight staff (80%) identified Equashield as the overall preferred CSTD, whereas two staff (20%) did not have a preference between Equashield and PhaSeal (i.e. they preferred both equally).
Work Health and Safety
The WH&S team identified that the steps most likely to cause worker injury were the connection of the syringe to a vial and inserting the secondary/extension set into the fluid bag. This was due to the force required, the twisting motion, and the repetitive nature of the process.
Both CSTDs required a similar linear application of force, PhaSeal 4.71 kgf and Equashield 5.89 kgf to connect the syringe to the vial. In contrast to Equashield, the PhaSeal system required force and a twisting motion to push the syringe onto the vial adaptor, which added significant strain to the compounder’s hands and wrists.
The PhaSeal secondary set (C100) has a fluted cut out extending approximately one-third of the length of the spike. The length of the fluted cut out is considerably less on the Equashield extension set (SA-1E). Observation and interviews with staff demonstrated PhaSeal required less force and twisting to insert the secondary set into the fluid bag compared to the Equashield extension set. The WH&S team determined it is likely the reduced fluted cut out contributes to the extra force needed to spike the bag with the Equashield extension set.
Other Benefits or Disadvantages
During the study staff perceived Equashield required fewer components during compounding with fewer items to spray/wipe into the CyDSC, the compounder had less consumables to open, and there was more space available in the CyDSC.
The PhaSeal system requires an assembly fixture to attach vial adaptors to vials. This fixture consumes a large footprint in the CyDSC. The Equashield system does not require this fixture.
Equashield syringe units have a closed back and are presented with factory sterile air. This sterile air is used to equalise the pressure between the vial and syringe when withdrawing medicine or reconstituting a vial. The Equashield syringe design negated the need to manually draw up air from the surrounding environment when compounding.
The IMP team identified a possible infection control benefit as the Equashield male connector, which is attached to a patient, is raised and easier to disinfect. The PhaSeal patient connector membrane is in a lower position housed within a raised outer plastic casing, making it more difficult to cleanse.
Another possible infection control benefit was identified with regards to the vial adaptor design. The PhaSeal vial adaptor has a large satellite air chamber offset to the side of the vial. This can cause the vial to unbalance and fall over, compromising the sterile critical connection point. In comparison the Equashield vial adaptors are smaller and symmetrical, and vials rarely fell over. The Equashield vial adaptor connection appeared easier to cleanse as the critical connection point is raised compared to the lower and enclosed connection point on the PhaSeal vial adaptor.
Equashield offers larger vial adaptors which can be used on vials that have a 23-mm vial neck (e.g. foscarnet) unlike PhaSeal.
The PhaSeal injector has a clear plastic window on the casing which allows visualisation of the enclosed retracted needle. The unit had difficulty with medicine flooding from the needle into the injector casing, resulting in lost dose. Compounders regularly changed injectors and had to replace the lost dose, which could only be done by opening the closed system. This issue was not identified with Equashield.
Similar to PhaSeal, it was identified the Equashield system was unsuitable to administer subcutaneous or intramuscular chemotherapy doses. The components were too bulky, difficult to use, the dead space volume would cause an unacceptable loss of dose (>10%), and it was too complex for parents and carers.
Whilst the trial only included preparing chemotherapy in infusion bags, the pharmacy team identified Equashield syringe units did not fit the B Braun syringe pumps used at the hospital. This contrasts with the PhaSeal CSTD system as it uses standard Becton Dickinson syringes, which are compatible with the B Braun syringe pumps.
The dead space or priming volume of both CSTDs had to be considered during the trial. The compounding unit calculated the volume loss in all CSTD components used during compounding to ensure the volume of medicine lost was not less than 10%.
Discussion
Equashield offered benefits when compared to PhaSeal to compound chemotherapy in the hospital pharmacy. The cost difference between the two CSTDs over a 6-month period was AUD $4684. Although Equashield was more expensive, this was offset by potential financial savings such as improved compounding efficiencies, decreased bung contamination, and the reduced risk of repetitive strain injury for staff members.
On average the study showed that when using Equashield instead of PhaSeal™ there was an approximate time saving of 1 min per product. Whilst seemingly insignificant, because the compounding unit produces on average 900 chemotherapy products per month, this translates to a potential time saving of 15 h per month.
A previous study into bung contamination when using PhaSeal by the hospital pharmacy compounding unit demonstrated a rate of rubber core bung contamination of 72 items per 100 000. While using Equashield the contamination rate was 16 items per 100 000. The previous study looked at contamination when compounding both infusions and syringes, and did not include compounding using vials with a smaller 13-mm neck size. The sample size in this study was less, with 1839 infusions compounded as opposed to 3877 products in the previous study. Equashield may decrease the chance of bung contamination when compared to PhaSeal.
The survey demonstrated staff preferred Equashield, but only three questions out of 13 achieved statistical significance. The preference towards using Equashield was similar to a previous study where the technicians scored Equashield higher than PhaSeal. Just prior to, and during the trial, three new staff members were trained to use both systems. All three staff members reflected that learning to use Equashield was easier than learning to use PhaSeal. All staff reported Equashield was faster to use. As to which system was preferred, eight staff answered Equashield and the other two did not voice a preference towards either Equashield or PhaSeal.
The only question where there was a trending higher rating for PhaSeal was inserting the secondary/extension set into the infusion bag, probably due to the increased force needed to insert the Equashield extension set into the infusion bag, an issue also highlighted by the WH&S analysis. This problem could be reduced with the use of alternative infusion bags or if the spiking technique incorporated sterile alcohol wipe lubrication of the spike prior to insertion.
The WH&S team determined that Equashield provided a less stressful option for engaging/disengaging the syringe and the vial adaptor, and is the preferred system for this step. PhaSeal’s fluted spike provided a better option for inserting the secondary set into the infusion bag. Overall, the WH&S team recommended Equashield given its capacity to remove the twisting component and reduce the ergonomic risks associated with connecting the syringe to the vial.
Multiple comments outside of the six key characteristics were noted. Time-saving benefits were attained by having fewer components to spray and wipe into the CyDSC and the CyDSC is less cluttered, vials with Equashield attachments are more stable and easy to cleanse, and the injectors do not flood. This may explain why products are quicker to compound with Equashield and why staff are more satisfied with Equashield.
The IMP team opinion needs further study and justification to determine if the theory of improved infection control with respect to cleansing male adaptors translates into an evidence-based benefit. Since Equashield requires fewer compounding steps this could decrease the chance of product contamination. Similarly, using closed-backed Equashield syringe units that contain factory sterile air could also offer an infection control benefit.
The issue of the Equashield syringe unit not fitting the B Braun syringe pumps requires further investigation. The incidence of chemotherapy infusions given via syringe pumps is infrequent and it may be appropriate to continue using Becton Dickinson syringes with an Equashield female connector (FC-1), similar to the PhaSeal CSTD design.
Limitations
This study ran for a 4-month period, which may not have been sufficient time to fully compare the two CSTDs. Ideally the time-in-motion part of this study should have included more than 21 items.
Only chemotherapy in infusion bags were compounded using Equashield. Ideally, the comparison study should have included the compounding of all products and administration. The opinion of nursing staff, administration costs, cytotoxic surface contamination in ward areas, and a WH&S review of nursing chemotherapy administration would also strengthen comparison results.
Conclusion
Although both CSTDs maintained non-detectable cytotoxic surface contamination levels, Equashield may be a more suitable alternative CSTD to PhaSeal. There are increased cost implications using Equashield, but the time taken to compound products was reduced and bung contamination appeared to be reduced. Equashield was the preferred system to reduce the risk of worker injury and staff preferences favoured Equashield.
Acknowledgements
The author would like to thank members of the pharmacy compounding unit team who participated in the research.
Conflicts of Interest Statement
The author declares that she has no conflicts of interest.
Authorship Statement
Evonne Katherine Smith: Conceptualisation; data curation; formal analysis; investigation; methodology; project administration; resources; software; validation; visualisation; writing – original draft; writing – review and editing.
Ethics Statement
This project was exempt due to the local policy requirements that constitute research by the Children’s Health Queensland Research Ethics Committee (Reference no: EX/23/QCHQ/97690). The justification for this ethics exemption was as follows: the study conformed with the National Health and Medical Research Council Ethical considerations in quality assurance and evaluation activities and met local requirements for a quality assurance activity and did not involve any assessment of staff. Informed consent was obtained from all staff via verbal explanation of the project and their voluntary participation. Staff consented via completion of the voluntary survey.
Funding Statement
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.